
A quasi-experimental study on a co-production- and school-based psychosocial well-being program in Hong Kong

In recent years, the co-production approach has gained traction as an effective strategy for enhancing psychosocial well-being among youth1,2,3,4,5,6. This research, using a quasi-experimental design, examined the effectiveness of “Healing Space,” a pilot psychosocial well-being program employing co-production for secondary school students in Hong Kong. By actively involving students in the co-creation of mental health spaces with their teachers and program facilitators, Healing Space aimed to foster positive mental health attitudes, enhance psychological well-being, and strengthen social connectedness within the school. Grounded in Self-Determination Theory7the initiative emphasized autonomy, competence, and relatedness, offering students a transformative experience that shifted their role from service recipients to active contributors. The following paragraphs introduce the definition of co-production, its theoretical relevance, the challenges associated with its implementation, and the design and delivery of Healing Space in local school settings.
Co-production and psychosocial well-being
Initially proposed in the public administration field for the design and delivery of public goods8,9in the field of psychosocial well-being, the co-production approach involves a combination of activities between service providers and users, necessitating the active engagement of all key stakeholders in creating psychosocial or mental health-related programs or services5,8,9. The first element of this approach lies in recognizing service users as assets rather than liabilities9. This approach shifts power from service providers to users5,9acknowledges participants’ capabilities, and empowers them to maximize their potential and strengths through the co-created intervention process5.
Another radical element in co-production is the blurring of roles between service users and professionals5,9. When service users are also recognized as professionals who have unique strengths, skills, and knowledge, professionals must consult users in service design and delivery—and users, in turn, actively contribute to shaping those services. As a result, the power hierarchy between professionals and service users diminishes, creating a level platform for meaningful collaboration among all stakeholders. Furthermore, professionals are referred to as facilitators rather than service providers, thereby changing the traditional top-down service delivery model5.
This leads to the third transformative element of co-production, which is the emphasis on reciprocity5,9. As service providers and users share equal power in collaborative service design and delivery, both have to be actively involved in the process5,9instead of placing service users under the spotlight as the “problem to be fixed,” co-production requires service users to actively contribute to the services designed and provided for the promotion of their community well-being. Hence, it underscores the reciprocal relationships between professionals and service users.
Evidence has been accumulating on the benefits of co-production-based mental and psychosocial health programs globally. Slay and Stephen (2013)5 found that mental health interventions using co-production were effective in promoting psychological health, enhancing social relationships, and reducing stigma towards mental illness among service users. Other youth interventions1,2,3,4 that emphasized children’s rights and actively involved young people in service co-planning were also found to reduce youth self-stigma related to mental illness and promote their mental health literacy. Additionally, a family- and intergenerational-based mental health program in Pakistan strengthened youths’ psychological resilience by inviting them to co-design a health promotion program that addressed their family-related hardships6.
Self-determination theory
The design and implementation of co-production-based psychosocial and mental health programs can be traced to Self-Determination Theory, which posits that autonomy, competence, and relatedness are fundamental elements of psychosocial well-being5,7. In co-production, autonomy refers to the freedom and choice that service users have over their contributions in service co-planning and co-delivery5,7. Competence refers to the ability to create an impact in their own lives and the lives of others through the active engagement of service users in co-designing and co-delivering services10,11,12,13. Relatedness refers to the ability to form meaningful relationships with others for shared goals. The integration of Self-Determination Theory eventually fosters attitude change, self-compassion, and social connectedness through the co-production approach5,10,11,12,13. Figure 1 illustrates the pathways from co-production to positive changes in mental health attitudes, self-compassion, and social connectedness through the intertwined psychological processes of autonomy, competence, and relatedness.
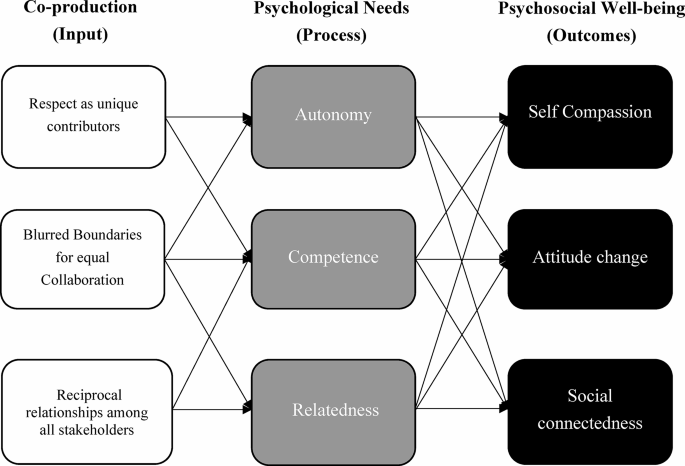
Conceptualizing theory of change from Coproduction to Psychosocial well-being.
Self-compassion can be cultivated by fulfilling the needs for autonomy, competence, and relatedness. Individuals experience autonomy when they are included in co-creating unique solutions that impact their lives. The inclusiveness in co-production empowers service users by respecting their unique skills and knowledge. By offering service users the freedom to make choices for themselves and improve their community’s well-being, they develop a sense of self-appreciation, leading to increased self-compassion14,15. This sense of autonomy is tied to the sense of competence through mastery experiences in co-implementing targeted mental health services. Recognizing their unique insights and abilities confirms their belief that they are capable of creating social impact, leading to a sense of competence, which correlates with self-compassion10,15. Co-production further offers a platform for relatedness by providing participants with opportunities to share their pains with others through the reciprocal exchange of experiences, cultivating self-compassion by knowing that “I am not alone in my suffering.”15 Moreover, the equal collaborative process of discussing and modifying targeted services with other stakeholders encourages interpersonal relatedness by embracing and understanding other people’s perspectives and experiences, thus fostering compassion for self and others.
Changes in mental health-related attitudes are driven by the co-production process in fulfilling autonomy, competence, and relatedness needs. Mastery experiences of co-producing mental health-related programs or services with other stakeholders on an equal platform lead to a sense of autonomy and competence in service users, making them influential members of their community and enabling them to make choices for themselves. These enabling experiences can disconfirm individuals’ hopeless perceptions about their current situation, thus inducing a positive attitude change regarding mental health-related matters. Furthermore, the process of co-producing a common goal encourages the exchange of perspectives among stakeholders10. Fulfilling collaborative relationships can offer new information to service users about the social world they live in, with community members embracing and accepting traditionally stigmatized mental illnesses5,16. For example, programs that employ a co-production strategy have been shown to reduce participants’ levels of mental illness stigmatization by engaging them in exchanging perspectives with professionals and cultivating their competence in making positive changes for their community5,10,16.
Social connectedness is fostered through promoting collaborative relationships between service users and providers and offering a social platform for service users to make decisions and impact their mental health with other stakeholders5,7. The inclusive and equal community for co-production cultivates shared values for relatedness among stakeholders17,18,19,20. The co-created social network that aims to strive for the common goal of mental well-being will facilitate service users’ perceived social support, foster a sense of community belonging, and contribute to the development of a close-knit community15.
Challenges in co-production
Nevertheless, challenges exist in the implementation of co-production in mental and psychosocial health programs. The most obvious barriers arise from the fundamental shifts in the dichotomous roles of service providers and users, which require extensive training14mindset changes, and humility from traditionally trained professionals. Co-production programs that lack the support and engagement of all stakeholders often result in limited impact on population well-being—and may even backfire due to clients’ unmet expectations and disappointment14. Even with the endorsement from service providers, different stakeholders may have varying expectations and understandings of their contributions, leading to confusion and potential conflicts21,22,23. Moreover, inequity exists in co-production programs. Users who are traditionally labeled as the vulnerable population often feel unsafe sharing their ideas due to the fear of being judged by others, leading to disengagement and inequality21,22. While worthwhile, our team was mindful of these limitations and potential challenges during the design and implementation of Healing Space.
The Hong Kong context
In recent years, the mental health of students in Hong Kong has been at an alarming state, with nearly 20% of students reporting suicidal ideation and 16% struggling with mental health issues24,25,26. The global COVID-19 pandemic, the resumption of schools post-pandemic, a top-down examination-oriented education system, and typical developmental transition challenges during adolescence have all contributed to poor mental health among students24,26,27. In Hong Kong, social stigma and fears of being labeled further prevent students from seeking help28,29,30.
Research conducted by the first author also showed that students lacked confidence and experienced fear when pursuing their desired futures, suggesting low levels of psychological resilience31. Information collected via pilot focus group interviews regarding school mental health further revealed that these young people did not prioritize their psychological well-being and had low levels of self-compassion31.
To promote school mental health and prevent further deterioration of students’ well-being, the Hong Kong government launched the “Mental Health@School” initiative, featuring the “Spread the Love, Care and Shine” campaign and a “Mental Health Literacy” online resource package for local schools32. To facilitate the design of customized school programs, the Education Bureau allocated a one-time grant to each local primary and secondary school to implement various mental and psychosocial health initiatives33. However, an education culture that prioritizes academic success and a high level of mental illness stigmatization have made school mental health programs difficult to implement30,34. Furthermore, these resources were offered in a top-down manner, which did not value students’ input in co-creating school mental and psychosocial health initiatives22. The professional-oriented strategy overlooked the need to view mental health issues from the students’ perspective, positioning them as the “problem to be fixed“22. To fill this service gap, we referenced current co-production literature1,2,3,4,5,6 to design Healing Space, a school-based and co-production-based psychosocial health program for Hong Kong schools.
The intervention: Healing space
Based on existing evidence and theoretical foundations on co-production5,7,15we conceptualized Healing Space to change students’ mental health-related attitudes, enhance self-compassion, and promote social connectedness within the school. This is achieved by actively engaging students in co-producing positive mental health-related interactive art installations with their teachers and program facilitators. These installations focus on the theme of promoting awareness of positive mental health by providing a space for students and teachers to feel relaxed and happy (Fig. 2a and b).

Installations of Healing Space.
Program guideline
The co-production-based mental health workshops were delivered by registered social workers and program facilitators in school settings, with each session designed to achieve specific outcome (Table 1). Students who directly participated in these six workshops with the goal of co-creating their mental health art installation were identified as co-producers. These co-producers were randomly selected by their schools based on their classroom grade (i.e., grade 8, 9, or 10) as a unit for recruitment.
The six workshops began with a professionally led approach and gradually transitioned to a peer-led format with co-producers leading the production of their art installations. The making of mental health-related installations was co-facilitated by social workers and a child psychologist with expressive arts training. For more complex installations, a design specialist was hired to support the students in completing their work. At the final exhibition, the co-producers displayed their mental health-related installations in various locations within their schools for their schoolmates, i.e., service users. These service users, who did not join the six workshops, were invited to participate in the final exhibition to interact with and test out these mental health installations created by the students who served as co-producers. Both co-producers and service users received regular psychoeducation classes embedded in their school curriculum.
As illustrated in Table 1, each workshop session started with a check-in activity in which students were invited to express themselves through movements, sounds, or an image to represent their emotional or physical status, followed by the core activity. Please see Table 1 for additional details on the activities that facilitators can choose from based on their observation of students’ needs during the session.
Fidelity
We embraced the co-production approach throughout the program’s conceptualization, design, and delivery. During the initial conceptualization stage, we collaborated with a local non-profit organization known for its extensive knowledge of frontline youth practices to co-design the framework of Healing Space. At the design stage, we engaged school management and teachers to discuss each session, ensuring that Healing Space met the specific needs of individual schools and their students. This approach also ensured program fidelity by requiring all program facilitators to align themselves with the program and school expectations. The program guideline, including the intention of each session and the range of activities, was available for all program facilitators.
A standardized half-day training was offered by a registered expressive arts therapist and another half-day was offered by a design thinking specialist before the program launch to align facilitators’ expectations and attitudes. During the program, the Principal Investigators also regularly met with the team to discuss and monitor the progress of each session. An expressive arts therapist also conducted two supervision sessions to address implementation challenges and ensure program fidelity.
Adaptations and variations
On the other hand, apart from having an overall framework and protocol, we also allowed our program facilitators to adapt the program details to fit the specific needs of the students at each site and the available resources at each school. While the guiding framework of the program is informed by Western literature, Healing Space was designed to fit the local educational context. The co-production approach was specifically adopted to empower students with a sense of autonomy to support positive mental health, particularly within Hong Kong’s examination-oriented, unidirectional education system, where students often feel disempowered within local school settings. Thus, Healing Space is a locally developed program—grounded in international theory but tailored to the local context.
Research aims and hypotheses
This study examined the effectiveness of Healing Space in promoting positive mental health attitudes by decreasing participants’ self-stigma related to mental illness (Aim 1), increasing self-compassion (Aim 2), and enhancing social connectedness (Aim 3).
For self-stigma, students in the service co-producer group and service user group will exhibit a faster rate of decrease in self-stigma related to mental illness compared to those in the control group (H1).
For self-compassion, students in the service co-producer group and service user group will experience a faster rate of increase in self-compassion compared to those in the control group (H2).
For social connectedness, the service co-producer group and service user group will experience a faster rate of increase in perceived classmate support, perceived teacher support, and a sense of school belonging compared to those in control schools (H3).
Within the experimental group, co-producers will show faster rates of change in all variables of interest compared to service users (H4).
link



