
Psychosocial interventions in palliative and end-of-life care

How to use psychosocial interventions effectively to enhance quality of life for palliative patients
Abstract
Providing non-pharmacological interventions that aim to minimise distress and relieve symptoms can greatly enhance the quality of life and death for people experiencing challenges associated with life-limiting diagnoses. Psychosocial interventions are particularly beneficial in supporting total pain, which includes the physical, psychological, social and spiritual aspects of distress. This article, the seventh in our series on palliative and end-of-life care, focuses on interventions that could benefit individuals receiving palliative care and their significant others. These are communication strategies, life story work, art therapy, animal-assisted interventions, relaxation techniques, multisensory stimulation and spiritual care.
Citation: Daly R, Drain D (2024) Psychosocial interventions in palliative and end-of-life care. Nursing Times [online], 120; 12.
Author: Rachel Daly and Diane Drain are academy lead Admiral Nurses, Dementia UK.
- This article has been double-blind peer reviewed
- Scroll down to read the article or download a print-friendly PDF here (if the PDF fails to fully download please try again using a different browser)
- Click here to see other articles in this series
Introduction
The psychosocial consequences of terminal illnesses are well established. Palliative diagnoses affect the emotional, physical, spiritual and social wellbeing of individuals and their families; however, despite many non-pharmacological interventions offering promising symptom management, psychosocial interventions in palliative care are underused by health professionals (Cardoso et al, 2023).
Providing psychosocial interventions can enhance the quality of life and death for people with palliative conditions. Although some interventions require a trained facilitator or practitioner and a specific implementation setting or context, many approaches and programmes can be effectively implemented by nurses and other health professionals to meet individual care needs or fulfil personal health objectives.
This article highlights some of the psychosocial interventions that are more commonly used in palliative and end-of-life care, with suggestions of how they can be implemented by nurses to maximise quality of life and reduce distress for patients and their care partners. Using these interventions can also greatly improve the wellbeing and job satisfaction of the health professionals themselves, as they witness the positive outcomes and benefit from the relationship and interaction that is central to their success.
What are psychosocial interventions?
Psychosocial interventions are evidence-based non-pharmacological approaches to care that aim to minimise distress and manage symptoms to optimise an individual’s quality of life (LeMay and Wilson, 2008). Each intervention is tailored to the individual, and integrated into their life and care plan, as necessary. These interventions involve collaborating with the participant and their care partners to provide a safe, therapeutic partnership that assesses and balances benefits against risks. Psychosocial interventions are recognised as relevant and safe solutions for palliative care (Teo et al, 2019).
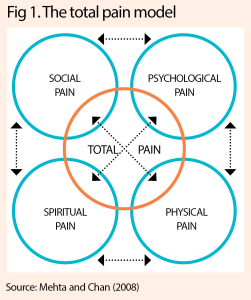
Psychosocial interventions are particularly useful in addressing needs that extend beyond physical symptoms to encompass the concept of ‘total pain’, which Dame Cicely Saunders originally defined in 1964 (Saunders, 2006; Richmond, 2005). Total pain refers to the proposition that a person’s experience of suffering encompasses not just physical pain, but also emotional, social and spiritual distress – all of which are interconnected and must be addressed for holistic care to be achieved (Fig 1).
The medical model often prioritises physical care and risks people feeling isolated, with their other – albeit equally important – needs unmet, so think about asking: “What do I need to know to give you the best care I can today?” It is imperative for nurses to adopt a holistic approach to palliative and end-of-life care, as emphasised by Cadet et al (2016), ensuring that psychological, social and spiritual rituals and care practices are also addressed. This approach recognises the interconnectedness of elements that affect pain, and aims to provide comprehensive support and comfort to people who are facing life-limiting conditions.
Assessment and care planning
It is important to think through interventions before implementation. They should be designed, adapted and tailored to the needs of the person and their care partners. These interventions may be non-pharmacological, but that does not mean they are free of effects that could potentially have a negative outcome for the person, such as increased pain or distress.
Any interventions should be delivered with therapeutic intentions. The following considerations may help to assess the suitability of the intervention and whether it could be successful:
- Is it appropriate for this person and their needs?
- Is the context (location, setting, timing) suitable?
- Are there any contraindications? If so, what are they?
- What is the duration (both the length of each session and the number of sessions proposed)?
- What is the planned frequency?
- Do you have the necessary training or knowledge (if appropriate)?
- Are the resources (human, financial and/or material) available to implement the intervention?
- How will the benefits (enjoyment, reduced pain or distress, better sleep) be assessed? Take note of the fact that benefits may be observed immediately or over time.
Person-centred care
The term ‘person-centred care’ is used in many spheres of health and social care. It describes a set of values that include tailoring care to an individual’s preferences, needs and values, with a focus on their life story, culture, identity, preferences, characteristics, interests and relationships.
Person-centred palliative care extends beyond addressing physical needs to encompass total pain, as described above. Knowing the person well is necessary to be sure care is provided with them in mind, especially when they may no longer be able to express their preferences and needs. Care partners can add valuable insight to guide individualised care.
Interventions
We will consider different psychosocial interventions that can be used to increase wellbeing and quality of life, including:
- Communication strategies;
- Life story work;
- Art therapy;
- Animal-assisted interventions;
- Relaxation techniques;
- Multisensory stimulation;
- Spiritual care.
Communication strategies
Palliative and end-of-life care presents many sensitive issues, so it is important that therapeutic communication is delivered in an effective and sensitive way (Cain et al, 2018). It is more challenging to communicate, however, when a person’s emotions are high. Emotions associated with elements of total pain may manifest in behavioural changes, such as displays of anger, guilt, crying and desperation. These emotions use a lot of energy and cannot be sustained for long periods, so initial approaches to therapeutic communication should be aimed at reducing the intensity of emotions and offering support in all the elements of total pain.
Two aspects of therapeutic communication that can help build robust and trusting relationships are:
- The art of silence – this can be purposeful, allowing the person to reflect on their illness and the impact it is having on them. The skill is not in filling the void, but in giving time and space to the silence, and recognising any non-verbal cues (Nicol and Nyatanga, 2017);
- The skill of empathy – true empathy is the ability to emotionally understand how the other person feels and experience the situation from their perspective. Empathising can increase rapport and the disclosure of more information, which can lead to a better understanding of a patient’s total pain and how to address it.
Life story work
Many people nearing the end of their life demonstrate psychological distress (Skinner et al, 2019). Life review is a person-centred care technique that uses the communication strategies discussed above to support people through this distress. It comprises structured questions that encourage people to reflect on and process their life experiences, aiming to find meaning by creating their life story, which can positively affect their quality of life (Elfrink et al, 2018).
Despite the benefits of life review, it is rarely used in palliative care as most palliative care practitioners have had little training in the technique. It is most often undertaken by trained therapists or psychologists, or in dementia care. Obtaining a story can be challenging and will depend on what the person chooses to talk about; this can vary greatly, depending on how moments, episodes and phases have affected their life.
When people are faced with a palliative or end-of-life situation, they may be more willing to discuss the many dimensions that make up their personhood. A qualitative study by Skinner et al (2019) identified four main themes that people talk about when reflecting on their lives:
- Life events;
- Values and beliefs;
- Family and support systems;
- Current medical conditions.
This provides a useful framework for health professionals to explore these themes, using an informal interview technique as they build relationships with patients. Enabling people to create their life story in this way may support them in the transition into end-of-life care.
Art therapy
Art therapy has emerged as a valuable intervention, offering holistic support to people facing life-limiting illnesses and end-of-life issues. By engaging in creative expression through various art modalities – such as painting, drawing, sculpture, collage, poetry, drama, expressive writing, dance and movement – people can explore and communicate complex emotions, fears and existential concerns that may be difficult to articulate.
Some forms of art therapy provide a non-verbal means of expression, making it accessible to people who may struggle with verbal communication due to physical or cognitive impairments. Research indicates that art therapy in palliative care settings can help alleviate symptoms such as pain, anxiety, depression and existential distress, while also enhancing quality of life, coping mechanisms and spiritual wellbeing (Fancourt and Finn, 2019; Chatterjee et al, 2018). In addition, art therapy can be used to preserve autonomy and self-expression, empowering people to retain and reclaim a sense of identity and meaning, despite illness and loss (Lefèvre et al, 2016).
Art therapy in palliative care is predominantly delivered by qualified art therapists, who possess clinical expertise and understanding of the therapeutic potential of creative expression (Wood et al, 2019). However, where art therapists are not available, integrating more generalised art interventions into palliative care programmes can address holistic needs for some individuals and promote psychosocial wellbeing.
Animal-assisted interventions
Animal-assisted interventions are known to offer unique psychosocial and emotional benefits to some people facing life-limiting illnesses. Animals, such as therapy dogs or cats, can provide comfort, companionship and a source of unconditional support to people during their end-of-life journey.
Research has shown that interactions with therapy animals can help reduce symptoms of anxiety, depression and loneliness among palliative care patients, while also enhancing their overall quality of life and wellbeing (Waite et al, 2018). Animals can also facilitate social engagement and emotional expression, enabling people to connect with others as they find solace in the presence of a non-judgmental and empathetic companion (Veilleux, 2021).
Animal therapy in palliative care should be implemented with careful consideration of individual preferences, while prioritising safety protocols and ethical considerations; it should also involve trained therapy animal handlers who adhere to professional standards and guidelines (Barker et al, 2019).
“Despite the benefits of life review, it is rarely used in palliative care”
Relaxation techniques
Relaxation techniques can offer holistic interventions that effectively target various aspects of total pain and distress for some individuals. Techniques such as mindfulness, music therapy and relaxation breathing exercises have shown significant benefits in palliative care settings. These techniques have been associated with reduction in pain, anxiety, depression and distress among people with life-limiting illnesses (Graham-Wisener et al, 2018; Carlson, 2013).
Music therapy involves the systematic use of music within a therapeutic relationship (Warth et al, 2015). In a palliative care context, music therapy can be used to facilitate spiritual support, effective communication and emotional regulation. It is increasingly recognised as a valuable psychosocial approach for managing behavioural symptoms, and promoting relaxation and comfort among individuals receiving palliative care (Moore et al, 2014).
Music therapy interventions – such as singing, active listening and playing instruments – can contribute to managing behavioural symptoms for people living with dementia (Moore et al, 2014). Research indicates that receptive or passive music therapy – such as listening to personalised playlists – offers calming effects even after the music has ended (Beer et al, 2012 ).
Therapy of this kind provides a shared non-verbal outlet for emotions for individuals and their care partners, thereby effectively addressing symptoms such as agitation, anxiety and aggression by facilitating emotional expression and emphasising dignity, respect and meaningful engagement in daily interactions (Pérez-Eizaguirre and Vergara-Moragues, 2021; Gold, 2014). Nurses can introduce music therapy while applying dressings or administering medications; they can also encourage families and carers to use it.
Multisensory stimulation
Sensory interventions – including approaches such as Namaste care – have emerged as promising strategies to promote quality of life in more advanced palliative care, offering holistic support to people facing advanced illness and end-of-life care (Lopes-Júnior et al, 2020).
Namaste care, designed for individuals with advanced dementia, incorporates sensory stimulation, gentle touch, soothing music, aromatherapy and other sensory experiences to create a calming and comforting environment. Research suggests that sensory interventions can effectively address symptoms such as agitation, anxiety and pain, while also enhancing quality of life and wellbeing for palliative care patients (Froggatt et al, 2020).
Sensory interventions provide opportunities for non-verbal communication, emotional expression and connection with others, fostering moments of presence, meaning and engagement at the end of life (Voetmann et al, 2022). They must be tailored to individual preferences and needs, with careful consideration of cultural, religious and personal beliefs.
Nurses have a key role in providing sensory care, and also in empowering families to use sensory stimulation in their interactions with the person who is dying. Examples of this could be providing hand or foot massage, using warm or cool flannels or towels, or introducing the sounds of birdsong or rainfall. By integrating sensory interventions, including Namaste care, into palliative care practice, nurses can offer compassionate and dignified support, promoting comfort, relaxation and connection in the final stages of life.
It is important to acknowledge that the evidence base for Namaste care is still evolving, and more rigorous research, including randomised controlled trials, is needed to establish its effectiveness. Despite this, the anecdotal evidence and the alignment of Namaste care with person-centred principles make it a promising approach in end-of-life dementia care.
Spiritual care
Spiritual wellbeing is an essential factor in end-of-life care (García-Navarro et al, 2021). Although spirituality and religion are often considered together, spirituality includes a broader existential belief system. Spirituality can be defined as a journey of self-discovery, giving the person a sense of meaning and purpose to their life (Richardson, 2014), while religion is an outward expression or practice of applying spiritual understanding or belief systems, values and rituals (Rego and Nunes, 2019). However, spirituality and religion are compatible, as they both include a search for the sacred.
It is useful to note that a person can be spiritual without belonging to a specific faith, belief or religion. Spirituality is always unique to the individual. It may be used in daily interactions and as a personalised support framework, holding different meanings for different people, and it may change as people journey through the phases of their life.
In palliative care, people can experience disruption of their beliefs and values system (Richardson, 2014), which can result in considerable spiritual distress and their potentially struggling to feel secure in sources of love, meaning and comfort, or experiencing conflict between their belief system and real-life events. It is therefore imperative that spiritual needs are recognised, understood and nurtured in end-of-life care.
Nurses can facilitate spiritual care by building on relationships, knowing the person and their care partners, and asking what is important to them and what needs to be prioritised. While nurses may not be able to facilitate faith rituals themselves, they can help care partners think about connecting with faith leaders that align with the patient’s needs.
Box 1 features a list of websites with further information about some of the approaches discussed in this article.
Box 1. Useful online resources
Conclusion
Providing non-pharmacological psychosocial interventions can minimise distress in palliative care. Such interventions are particularly beneficial when supporting the concept of total pain, which includes the physical, psychological, social and spiritual aspects of distress, creating a therapeutic space for a person-centred approach to palliative care.
These interventions must be tailored to the needs and abilities of the individual, recognising all the aspects of distress they might be experiencing. Nurses should always implement them with sensitivity and respect for the person’s dignity and autonomy. Involving family members and other care partners in the care plan and its delivery is not only essential for comprehensive support for the individual, but may benefit care partners’ wellbeing too.
- The next and final article in this series will explore the current guidance for care at and after a person’s death
Key points
- Psychosocial health in palliative care is a major concern linked with depression, anxiety and other mental health problems
- These interventions can be implemented by nurses
- Psychosocial interventions help reduce distress for patients and their care partners
- Accurate and holistic assessment and care planning will help determine the most suitable interventions
References
Barker SB et al (2019) Animal-Assisted Interventions in Health Care Settings: A Best Practices Manual for Establishing New Programs. Purdue University Press.
Carlson LE (2013) Mindfulness-based cancer recovery: the development of an evidence-based psychosocial oncology intervention. Oncology Exchange; 12: 2.
Nicol J, Nyatanga B (2017) Palliative and End of Life Care in Nursing. Learning Matters.
Saunders CM (2006) Cicely Saunders: Selected Writings 1958-2004. Oxford University Press.
Waite TC et al (2018) A meta-analysis of animal assisted interventions targeting pain, anxiety and distress in medical settings. Complementary Therapies in Clinical Practice; 33, 49-55.
Wood MJM et al (2019) The International Handbook of Art Therapy in Palliative and Bereavement Care. Routledge.
Help Nursing Times improve
Help us better understand how you use our clinical articles, what you think about them and how you would improve them. Please complete our short survey.
link



