
Evidence based recommendations for health professionals to improve care of people with spinal cord injury and cognitive impairment: an update to the psychosocial care practice guide

Themes, recommendations, and implementation strategies for cognitive impairment
Theme 1: Raise awareness of causes of mild to moderate CI and sub-types of CI in people with SCI when participating in rehabilitation
Recommendation 1: It is recommended that all staff and treating team members receive training to increase awareness of the likely occurrence of cognitive impairment following SCI
Given that a phase of intensive rehabilitation occurs after a SCI, treating staff being aware of a possible CI is essential, as it can significantly impact long-term rehabilitation outcomes. By raising awareness, the risk of poor rehabilitation outcomes can be mitigated, leading to more effective and tailored care for those with SCI [16, 26, 27]. Current evidence suggests that patients with SCI have substantially increased risk of cognitive impairment [16, 27,28,29].
Suggested implementation strategies:
-
(1)
Raise awareness by developing and distributing relevant materials for staff, treating team, people with SCI, their families, and the broader community to promote understanding and reduce stigma surrounding cognitive impairment.
Recommendation 2: It is recommended that healthcare providers understand and thoroughly assess all possible contributors to cognitive impairment in people with SCI
It is important to avoid assuming that cognitive changes in people with SCI are purely situational or reactive. Each person should be assessed thoroughly to understand the full scope of possible CI. CI may stem from a variety of underlying causes, including neurological changes associated with the injury itself. A thorough, individualised assessment allows HCPs to identify accurately and understand the nature of any impairment, ensuring that any cognitive challenges are addressed appropriately and effectively, rather than overlooked or misattributed. While comorbid traumatic brain injury (TBI) is a common cause of CI following a traumatic SCI [16, 18, 30,31,32], there are numerous other contributors or causes [31, 33, 34]:
-
severe mental illness or a psychological disorder (e.g., depression, anxiety, chronic stress, or alcohol and substance use disorder)
-
decentralised cardiovascular function
-
sleep apnoea
-
polypharmacy (e.g., use of opioids, anticholinergics)
Other possible contributors or causes that may impair cognitive function in SCI include [16, 34]:
-
injury or inflammation to CNS (other than TBI)
-
personal factors (e.g., age, sex, and education)
-
environmental factors (e.g., critical care, intensive hospitalisation, community transition)
-
secondary health conditions (e.g., chronic pain, fatigue).
People with SCI may experience significant cognitive challenges due to environment contextual factors. Sudden changes in the environment, social dynamics, and responsibilities can overwhelm people, impacting their cognitive function. For example, transitioning from hospital to the community (at first discharge) is often associated with increased anxiety and feeling emotionally overwhelmed [7, 35], which can contribute to temporary cognitive fluctuations or cognitive burden rather than true CI. However, prolonged exposure to stress and limited cognitive stimulation could contribute to cognitive difficulties if not addressed.
Suggested implementation strategies:
-
(2)
Develop educational materials and training programs for healthcare professionals to enhance their understanding of the causes and implications of mild to moderate CI in people with SCI.
Theme 2: Improve awareness of terminology of what constitutes mild, moderate, and severe CI in people with SCI and associated symptoms
Recommendation 3: It is recommended that healthcare providers use standardised terminology when defining mild, moderate, and severe cognitive impairment in people with SCI.
Research has shown there is a lack of understanding of what constitutes levels of CI in rehabilitation teams, so it is important to standardise terminology [36]. Clear and consistent language will enhance reliable communication across care teams and improve the accuracy of assessment and treatment plans. However, clinical judgment should be applied in conjunction with the definitions outlined below to ensure that the unique cognitive and functional needs of each patient are appropriately addressed.
-
a.
Mild CI can be defined as impairment in cognitive function (e.g., mild memory loss) in adults that is greater than expected for a person’s age and education level but does not significantly interfere with activities of daily life [37, 38].
-
b.
Moderate to severe CI in adults can be defined as a significant cognitive decline from a previous level of performance, greater than expected for the person’s age and education level, in one or more cognitive domains, such as memory, attention, perceptual-motor skills, language, social cognition, and executive function.
The severity rating should be based on the extent to which cognitive deficit/s interfere with independence and everyday functioning, potentially resulting in a loss of independence and a substantial need for assistance with daily tasks, such as managing finances and taking medications. It is important to identify sub-types of CI such as amnestic CI (primary memory impairment) versus non-amnestic CI (where non-memory domains dominate) [38]. The cognitive decline should not be attributed to delirium.
Suggested implementation strategies:
-
(3)
Establish a standardised set of terms and definitions related to CI after SCI to ensure consistent language for interpretation and communication across healthcare settings.
-
(4)
Disseminate the standardised terminology through educational resources, guidelines, and training programs to ensure widespread adoption among healthcare professionals.
Recommendation 4: It is recommended that healthcare providers develop a thorough understanding of the common signs and symptoms of cognitive impairment following SCI
Early recognition of signs and symptoms of CI is essential for understanding its impact on patients with SCI. CI can manifest in various ways [18, 19, 39], including the following:
-
a.
forgetfulness or memory loss
-
b.
low motivation and inaction
-
c.
difficulty with solving life problems
-
d.
difficulties communicating with slower processing of information and verbal response time
-
e.
trouble recognising familiar people and places
-
f.
problems with attention
-
g.
difficulty understanding or implementing multiple step instructions or tasks
-
h.
trouble exercising judgment, such as knowing what to do in an emergency
-
i.
difficulty planning and carrying out tasks
-
j.
problems with managing emotions and with adjustment, including elevated anxiety and depressive mood, frustration
-
k.
disorganisation.
Suggested implementation strategies:
-
(5)
Promote staff awareness through training modules or reference guides designed to help healthcare providers recognise the signs of CI (see Fig. 2).
Fig. 2 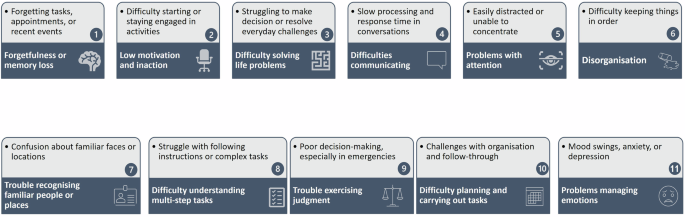
Infographic: Signs of cognitive impairment.

Recommendation 5: It is recommended to provide appropriate orientation and ongoing professional development opportunities for staff to acquire and maintain the necessary skills for effectively supporting people with SCI who have cognitive impairment
Structured, employer-assisted education and support programs should be developed for staff to be adequately resourced and skilled to effectively implement care for people with SCI at high risk or suspected of CI. In addition, support will be required to promote the continued use of these skills, such as access to supervision.
Suggested implementation strategies:
-
(6)
Professional development for detecting, assessing, and managing CI should also be offered, with regular evaluations and feedback to ensure the continuous improvement and application of these skills.
Theme 3: Describe best approaches to assessing CI in people with SCI, including screening processes, time points, assessment tools, and health professionals involved
Recommendation 6: It is recommended that an initial brief validated cognitive screening be conducted as soon as practicable following SCI, regardless of mechanism and level of SCI
Current evidence suggests that a person with SCI has substantially increased risk of CI [16,17,18,19]. Therefore, it is imperative to assess cognitive function in people with SCI during rehabilitation [16, 28, 39]. The purpose of the cognitive assessment using a validated screening tool is to ensure that the treating team is aware of any possible underlying level of CI that can impact on the process of rehabilitation through the continuum of care.
Recommendation 7: Conduct cognitive screening for patients upon admission to SCI rehabilitation and periodically throughout their lifetime to monitor any changes over time
Other considerations:
-
Valid and objective cognitive assessment should be conducted after the patient has settled into the rehabilitation phase, based on clinical discretion.
-
It should not be done on a patient if they are unwell. In this scenario, the assessment may be based upon their history as obtained from significant others (such as family members and general practitioner), regarding risk factors such as a previous history of psychiatric disorder. As soon as the patient can communicate, a direct assessment should occur involving them.
Recommendation 8: It is recommended that cognitive screening and psychosocial assessment be conducted for patients who are at a high risk of cognitive impairment or who have suspected co-morbid conditions (such as TBI) or other risk factors (such as, older age)
A psychosocial assessment of risk factors associated with CI should be conducted. Identifying CI in people with SCI is essential for developing tailored management strategies and be integrated into rehabilitation planning.
Suggested implementation strategies:
-
(7)
Develop guidelines and protocols for the comprehensive assessment of CI in people with SCI, incorporating validated assessment screening tools and procedures.
-
(8)
Provide training and resources for healthcare professionals on the administration and interpretation of cognitive assessment measures specific to SCI.
Recommendation 9: It is recommended that validated neurocognitive capacity screens be utilised
Valid neurocognitive screens can be important tools that can be used to detect the presence of mild to moderate CI after SCI. However, there are no validated neurocognitive measures created specifically for people with SCI [16, 19] including those with limited hand functions. Hence SCI Units should develop a regimen of validated cognitive capacity screens that could be used to determine the possible presence of CI after SCI [19, 25, 40]. Rehabilitation staff should receive training (such as from a neuropsychologist or clinical psychologist) in conducting cognitive screening and interpreting the results.
Accurate screening for CI in people with SCI is crucial for optimising rehabilitation outcomes. Despite its clinical importance, there is a notable lack of screening tools developed specifically for SCI, leading clinicians to rely on instruments validated in other populations. This creates a unique challenge, as many existing cognitive screening tests were not designed to capture the specific deficits seen in SCI. Cognitive performance in people with SCI may be influenced by a combination of injury-related factors, secondary health conditions, and neurological changes that differ from those typically observed in neurodegenerative disorders. The limitations in validity and applicability of currently available tools for CI screening in people with SCI are summarised as Appendix E.
Recommendation 10: It is strongly recommended that if the results of a neurocognitive screen indicate cognitive impairment, healthcare providers should consider referral for comprehensive neuropsychological testing depending on the individual case
Depending on the mechanism of injury and irrespective of level of injury, evidence suggests people with SCI should be screened for evidence of TBI (e.g., post-traumatic amnesia, Glasgow Coma Scale) when admitted to the emergency department and/or acute care to inpatient rehabilitation [41]. In cases where people with SCI are suspected to have sustained a TBI, the Abbreviated Westmead Post-Traumatic Amnesia Scale (or equivalent) should be administered on admission to ED or in acute care, where possible.
Theme 4: Define person-centred care (PCC) in the context of mild to moderate CI in people with SCI when engaged in rehabilitation
Recommendation 11: It is recommended that person-centred care (PCC) be prioritised when treating people with SCI who also has cognitive impairment
Focusing on the injured person’s unique needs, preferences, values, and circumstances is essential for delivering effective and compassionate care. This is achieved through a dynamic relationship among those who are important to them, and all relevant providers [42, 43].
PCC involves the SCI rehabilitation team engaging a person with SCI in a collaborative, flexible, encouraging, and sensitive manner, which will most likely result in improved SCI perceptions/ participation in rehabilitation for those with CI [44, 45]. Factors essential to PCC like trust in relationships, emotional intimacy, and participation encourage post-traumatic growth in people with a SCI [46].
Suggested implementation strategies:
-
(9)
Foster a PCC approach in the delivery of care, recognising the unique needs, preferences, and goals of people with SCI and CI.
-
(10)
Promote shared decision-making and involve people with SCI with CI in their care planning and goal-setting processes.
Theme 5: Develop a list of recommended ways to improve how SCI rehabilitation health professionals (and caregiver/family) verbally communicate to those with mild to moderate CI
Recommendation 12: It is recommended that verbal, language, and speech strategies be utilised to enhance communication with people with SCI and cognitive impairment
The use of cognitive support strategies may improve communication between rehabilitation staff when interacting with people with SCI and CI [47, 48]. Supportive and helpful language employing strengths-based approaches should be used when communicating with people who have mild to moderate CI after SCI. Some of the recommended general suggestions are presented as an infographic (Fig. 3).

General verbal communication strategies for healthcare providers when treating people with SCI and cognitive impairment.
Suggested implementation strategies:
-
(11)
Provide training to healthcare professionals on effective communication strategies tailored to people with SCI and CI.
-
(12)
Develop educational modules and communication aids and resources, such as visual supports, simplified language, and alternative communication methods, to facilitate effective (verbal) communication.
Recommendation 13: When engaging in verbal interactions with people who have cognitive impairment, it is recommended to avoid open-ended questions
When communicating with people who have CI, using open-ended questions can sometimes lead to confusion and hinder understanding. Instead, it is recommended to use clear, direct questions that guide responses, such as yes/no or multiple-choice formats, tailored to the person’s needs and abilities. Selecting the appropriate question type, the healthcare provider should consider factors like the patient’s severity of impairment, education level, literacy, and comprehension. For example, when reliable yes/no responses are possible, these can enhance clarity and reduce frustration, helping to create a more effective and supportive communication experience.
Theme 6: Develop a list of recommended ways to improve how SCI rehabilitation health professionals (also caregiver/family) non-verbally communicate to those with mild to moderate CI
Recommendation 14: It is recommended that non-verbal strategies, such as gestures, facial expressions, and body language, be utilised to enhance communication when needed
Effective communication is essential in healthcare settings, particularly when managing people with complex needs, such as those with cognitive or physical impairments. By incorporating non-verbal strategies, healthcare professionals can improve understanding, and ensure that critical information is conveyed accurately, especially in situations where verbal communication may be limited or ineffective [47, 48]. This approach supports PCC, ensuring that communication barriers are minimised. Some of the recommended suggestions are presented as an infographic (Fig. 4).

General non-verbal communication strategies for healthcare providers when treating people with SCI and CI.
Suggested implementation strategies:
-
(13)
Educate healthcare professionals on the importance of non-verbal communication cues and develop resources and training programs that focus on enhancing non-verbal communication skills.
Theme 7: Determine challenges and barriers to improve communication and care for those with SCI and who also have CI
Recommendation 15: It is recommended that clients receive timely and tailored information that aligns with their cognitive function status, ensuring accessibility and comprehension for effective self-management and care
A person admitted with an acute SCI requires timely and targeted information about medical diagnosis and prognosis of their SCI when it is deemed that they are ready. However, this needs to be done without overwhelming them. This is also crucial to their understanding of the processes involved in their rehabilitation. The person depends on accurate information to facilitate their active engagement in the discussion of treatment options.
Fluctuating clinical presentations, and the development of secondary health conditions, result in an on-going need for good quality information. Certainly, there is a need for information about diagnosis and prognosis to be repeated as necessary. Overcoming barriers to shared decision-making is important. There are a range of barriers and facilitators to effective shared decision-making. These may include the:
-
age, sex, culture, attitudes, opinions, level of education, and past experience of being a patients
-
health literacy
-
emotional readiness for partnering
-
degree of trust and confidence in the healthcare system and clinicians
-
communication style and skills of both parties.
Most common barriers are organisational structure/administrative supports (e.g., lack of decision trees for the condition or scenario) and lack of time to build relationships and trust and explore all the options, or a lack of available evidence, to allow informed decision-making. The following approaches have been found to augment shared decision-making:
-
actively supporting people to be involved in decision-making
-
emphasising options and problem solving
-
developing care plans as a partnership between patients and professionals
-
setting PCC goals and following up on the extent to which these are achieved over time
-
using decision aids rather than merely providing information
-
providing opportunities to share and learn from peers with the same condition.
Recommendation 16: Recognise that people with SCI and cognitive impairment may have difficulty sustaining a conversation due to problems with attention, processing information, and short-term memory
Short-term memory issues often intersect with other factors such as forgetting, distractions, and attentional difficulties, further complicating communication. This can further result in confusion, difficulty following conversations, and a need to frequently re-establish context or clarify information. To address these barriers, healthcare providers should adopt strategies that accommodate these limitations. These strategies include providing additional time for processing information, repeating key points as needed, and using supportive communication techniques to enhance understanding.
In addition, creating an environment conducive to focus is crucial. Minimising distractions can help the person better engage in the interaction. Structured aids, such as steps, checklists, written handouts, or visuals, can also support comprehension and retention. It is equally important to consider the impact of fatigue. Interactions should ideally take place when the person feels rested, alert, and not overwhelmed by tiredness.
Recommendation 17: Be aware that people with SCI and cognitive impairment may quickly forget information they have understood during conversations, which can hinder long-term retention and follow-up communication
People with SCI and CI may often struggle with retaining information shared during conversations, even if they initially understand it. This can lead to confusion and miscommunication, as they may not retain key details needed for decision-making or ongoing discussion. This can disrupt the flow of communication, as they might frequently lose track of what was discussed, making it challenging for them to follow or respond accurately. Identifying this challenge enables healthcare providers to support people by using methods like repetition, simplifying messages, and providing written or visual aids to reinforce understanding and facilitate clearer, more effective communication.
Recommendation 18: Ensure that people with SCI and cognitive impairment are provided with necessary adjustments, such as additional time or written reminders, to support their full participation in treatment and decision-making processes
Providing adjustments like additional time to process information, written reminders (visuals or handouts) for key details, and simplified instructions can significantly enhance people’s ability to understand and participate in their care. These supportive measures not only promote independence but also promote a more inclusive environment where people feel empowered and engaged in their treatment journey, leading to better overall outcomes.
Recommendation 19: Understand that people with SCI and cognitive impairment may face communication challenges that lead to frustration, negative moods, and behaviours, which can further hinder effective communication and engagement
Difficulties in expressing thoughts and needs may cause the person to feel isolated or unheard, intensifying their frustration. Recognising these emotional responses enables healthcare providers to respond with empathy and patience, using strategies that promote calm and understanding, thereby reducing barriers and supporting a more positive communication experience.
Suggested implementation strategies:
-
(14)
Conduct research and gather feedback from people with SCI, healthcare professionals, and stakeholders to identify common challenges and barriers to effective communication.
-
(15)
Use the findings to inform the development of targeted interventions, policies, and support systems to address these challenges and promote improved communication outcomes.
Recommendation 20: Recognise and consider system-level barriers and facilitators that may impact the implementation of the recommended strategies
A list of potential barriers and facilitators are presented in Fig. 5 that may arise when implementing the above recommendations in clinical practice [49].

Potential barriers and facilitators when implementing the recommendations.
link



